Topic: Converting lab test results from measurement values to meaningful grades
Problem: When patients get results from their bloodwork or other lab test, they do not get a clear idea of the actionable meaning of each test result. Each test result is shown as a value, with its dimensional units, and often, an indication of how that value compares with the “normal” range. The patient does not get any idea of the measurement’s import or what the clinician will suggest to do about that result.
Suggested Solution: Do the same for lab test results across all lab tests as we do for cancer. Oncology uses a standard “stages” (I, II, III, IV) grade scale for cancer, used by physicians and patients across all cancers, throughout the health care world. Create a grade scale for lab test results.
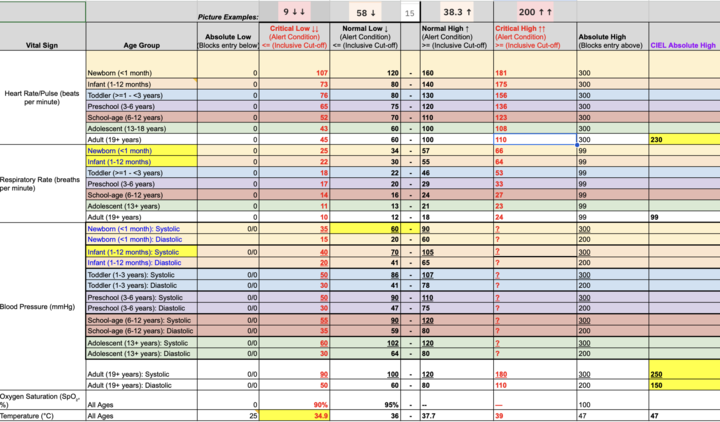
Proposal: Seven-level set of grades for lab test results with consistent meanings and implications:
-
Severely below normal: Must treat urgently
-
Below normal: Treat
-
Low normal: OK. Monitor more often
-
Normal: Be happy. Test periodically
-
High normal: OK. Monitor more often
-
Above normal: Treat
-
Severely above normal: Must treat urgently
On the lab test results report, the grade for each test result could be printed on the same line as the measurement value and the same-line range chart.
Value of this grade scale: Patients and clinicians have a concept of the grades and the actionable implications. A finer scale, such as one with 10 steps, does not explain the semantic difference between, say, 6 and 7. A coarser scale does not include a different grade for each action.
Problem: Different clinicians may map measurements to these grades using different breakpoints.
However, this is only a problem where the clinicians have the independence to decide their own breakpoints. In many health systems, they do not.
Problem: Comorbidities and other individual differences change the grade appropriate to the measurement.
Solution: The clinician tells the patient his own professional assessment of the grade for the individual patient. The patient would still understand the meaning of the grade within the range of grades.
Questions:
- Is this reasonable?
- Does it need improvement?
- Is LOINC the channel to advocate for it?
- Where else?